The financial stability of modern healthcare organizations is under immediate threat. A quiet crisis is developing across the revenue cycle. Recent industry statistics reveal that the initial medical claim denial rate has escalated to an alarming 11.8%.
More than one in nine claims is denied on first submission, increasing workload, delaying payments, and impacting revenue cycle performance.
For a mid-sized health system or hospital group, this is not just an administrative burden. It represents a severe financial drain. Annually, an estimated $262 billion in US healthcare claims are denied on first submission. Even more critical is the fact that 65% of those denied claims are never reworked or appealed. They simply age out in accounts receivable (A/R), resulting in permanently lost revenue.
[Traditional Reactive Model]
Claim Submitted ──> Payer Denial ──> Manual Rework ($25–$181/claim) ──> 65% Abandoned
[AI Predictive Prevention Model]
Data Capture ──> AI Pre-Submission Scrub & Risk Scoring ──> Clean Submission ──> ~95%+ Approval
However, the underlying issue is no longer limited to human error; instead, it reflects a fundamental mismatch in capabilities. As payers continue to leverage sophisticated AI algorithms to scrutinize claims and identify denial risks, many healthcare providers remain dependent on legacy RCM platforms and manual billing processes. Consequently, this technology gap makes it increasingly difficult for billing teams to keep pace with evolving payer requirements and denial patterns.
Consequently, this gap creates significant operational challenges. Not only does it slow reimbursement cycles, but it also increases the likelihood of preventable denials. Moreover, the financial impact is substantial. While a clean claim typically costs about $6.50 to process, a denied commercial claim can require between $25 and $181 in additional staff time and administrative resources to rework. As a result, organizations face rising costs, reduced efficiency, and increased revenue leakage.
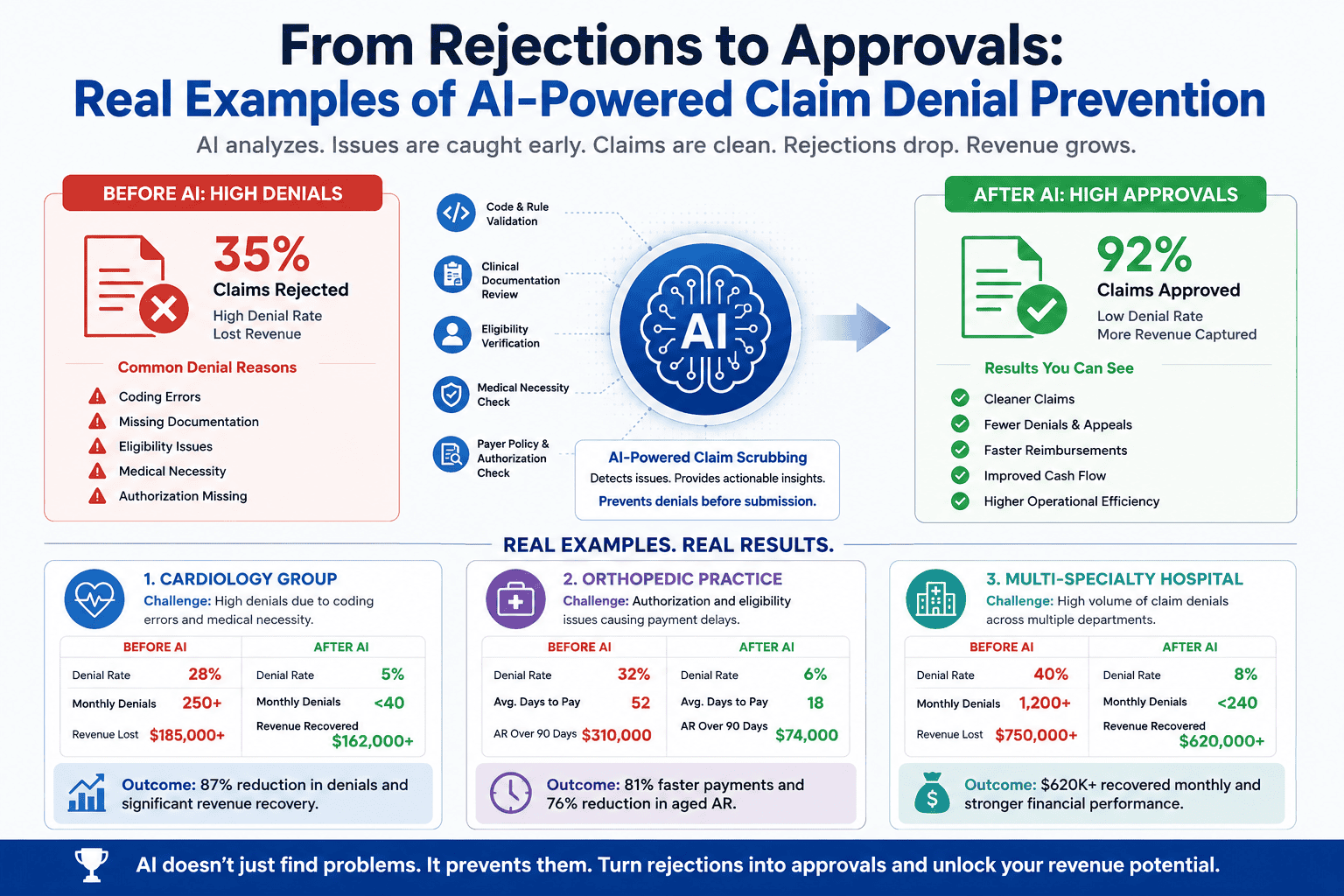
Fortunately, forward-thinking healthcare organizations are taking a different approach. Rather than reacting to denials after they occur, they are proactively leveraging AI-powered predictive analytics to identify and resolve issues before claims are submitted. Consequently, this shift enables providers to reduce denials, accelerate reimbursements, and improve overall revenue cycle performance.
Furthermore, as AI technologies continue to evolve, denial prevention is becoming increasingly precise and scalable. Therefore, this analysis explores real-world case studies, advanced machine learning frameworks, and proven AI strategies that are helping healthcare organizations transform claim rejections into consistent approvals.
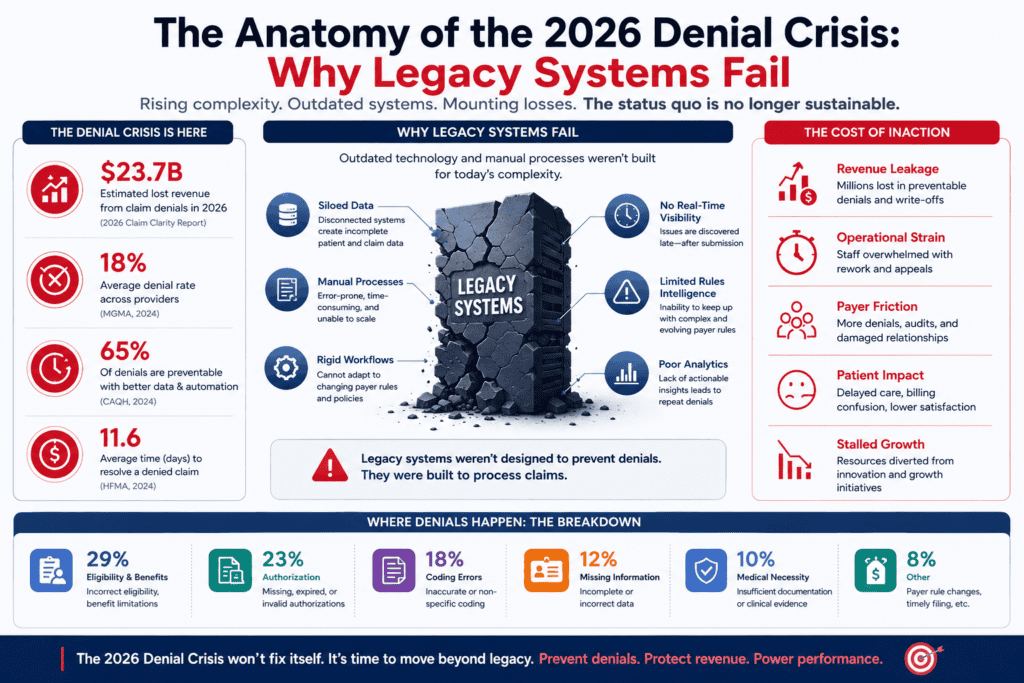
1. The Anatomy of the 2026 Denial Crisis: Why Legacy Systems Fail
To successfully deploy an AI-driven denial prevention solution, it is vital to understand why legacy rules engines—often called basic “claim scrubbers”—are no longer sufficient.
The Realities of Modern Payer Algorithms
Traditionally, claim scrubbers operate using static, hardcoded rules. In other words, they primarily validate basic claim elements, such as whether required fields are completed, whether a Current Procedural Terminology (CPT) code exists, or whether a member ID meets the expected format and character length.
However, the healthcare reimbursement landscape has evolved significantly. While providers often continue to rely on rule-based validation systems, modern health insurance payers are increasingly leveraging sophisticated machine learning algorithms. As a result, payer systems no longer depend solely on static rules. Instead, they dynamically evaluate clinical intent, documentation quality, medical necessity requirements, and utilization patterns in real time.
Consequently, a critical gap has emerged between how providers submit claims and how payers review them. For example, a payer’s system may approve a specific combination of an ICD-10 diagnosis code and a CPT procedure code on Monday. However, by Thursday, that same claim combination could trigger an automatic rejection due to newly updated medical necessity criteria, revised reimbursement policies, or localized payer-specific guidelines.
Furthermore, because these changes can occur rapidly and often without direct visibility to providers, billing teams frequently struggle to keep pace. As a result, legacy claim-scrubbing systems become increasingly ineffective. Since they rely on fixed logic rather than adaptive intelligence, they cannot recognize evolving payer behaviors or anticipate emerging denial risks.
Therefore, organizations that continue to depend on static validation tools often find themselves reacting to denials after submission rather than preventing them beforehand. In contrast, AI-powered denial prevention platforms continuously learn from payer decisions, enabling providers to adapt proactively, reduce denials, and improve first-pass claim acceptance rates.
The True Cost of Manual Intervention
When a claim is denied, the financial impact extends far beyond the delayed reimbursement. It sets off a highly inefficient manual workflow:
- Labor Drain: Certified medical coders and billing specialists must log into disparate payer portals, interpret vague Claim Adjustment Reason Codes (CARCs), and manually search the Electronic Health Record (EHR) for missing data.
- A/R Aging: The average time to resolve a manual appeal ranges from 45 to 90 days. This delay increases days sales outstanding (DSO) and restricts working capital.
- Write-off Accumulation: Due to strict timely filing limits and limited staff capacity, complex denials are often written off entirely, directly harming net margins.
The Interoperability Gap
Most healthcare enterprises operate within a fragmented technology ecosystem. The hospital EHR, the clinic scheduling platform, the standalone laboratory information system, and the clearinghouse portal frequently function in isolation.
Without a cohesive, intelligent layer to bridge these systems, critical data vanishes. A patient’s updated primary insurance, captured at a check-in desk, may fail to sync with the backend billing system in time. The result is an entirely preventable eligibility denial.
2. The Mechanics of AI-Powered Denial Prevention
AI-driven claim denial prevention does not simply clean up errors after the fact. It fundamentally restructures the data flow across the entire revenue cycle.
Furthermore, by integrating seamlessly with EHR and billing systems, the technology applies a multi-layered AI-driven approach to assess denial risk before claim submission, enabling proactive error detection and correction.
[Clinical Notes & EHR Data]
│
▼
┌───────────────────────────┐
│ Natural Language │ <-- Extracts clinical intent &
│ Processing (NLP) Engine │ matches medical necessity
└─────────────┬─────────────┘
│
▼
┌───────────────────────────┐
│ Predictive Risk Scoring │ <-- Evaluates claim against historical
│ (Machine Learning) │ payer patterns (Gradient Boosting)
└─────────────┬─────────────┘
│
▼
[Is Claim At Risk?]
╱ ╲
YES NO
╱ ╲
▼ ▼
┌──────────────┐ ┌──────────────┐
│ Routed to │ │ Autonomous │
│ Human Expert │ │ Clearinghouse│
│ Audit Queue │ │ Submission │
└──────────────┘ └──────────────┘
Deep Data Integration
The prevention process begins with comprehensive data ingestion. The AI system extracts unstructured data from physician clinical narratives, structured laboratory values, historical payment files (835 Electronic Remittance Advices), and active claim submissions (837 files).
This holistic view enables the platform to analyze the complete clinical context of a claim, rather than evaluating codes in isolation.
Natural Language Processing (NLP) and Clinical Intent
Furthermore, a significant percentage of claim denials arise from “lack of medical necessity” or “insufficient clinical documentation.” Traditionally, standard claim scrubbers have been unable to interpret a physician’s narrative notes. However, advanced AI-powered platforms are changing this approach by leveraging sophisticated Clinical Natural Language Processing (NLP) technology.
Specifically, the NLP engine analyzes unstructured clinical text, including operative reports, History of Present Illness (HPI) documentation, and physical examination findings. Subsequently, the system compares this information against the payer’s most current Local Coverage Determinations (LCDs) and National Coverage Determinations (NCDs).
As a result, the AI can identify documentation deficiencies long before a claim reaches the payer. For example, if a required clinical element—such as a documented conservative therapy trial period, specific diagnostic findings, or a minimum laboratory threshold—is absent from the medical record, the system immediately flags the gap.
Consequently, providers gain an opportunity to strengthen documentation before claim submission. Moreover, by addressing these issues proactively, healthcare organizations can significantly reduce medical necessity denials, improve first-pass acceptance rates, and accelerate reimbursement timelines. Therefore, instead of discovering documentation problems after a denial occurs, teams can resolve them upfront, leading to a more efficient and financially resilient revenue cycle.
Machine Learning and Predictive Risk Scoring
Rather than relying on human programmers to write compliance rules, the system trains machine learning algorithms on years of historical claims and remittance data.
For every claim prepared for submission, the machine learning model evaluates hundreds of discrete data features. These include the provider’s specialty, the specific payer, the combination of CPT/ICD-10 codes, modifiers used, the patient’s demographic profile, and the place of service.
The model outputs a precise Predictive Denial Score (ranging from 0% to 100%). Claims that exceed a specific risk threshold are automatically diverted from the automated submission stream and placed into a specialized human review worklist, accompanied by a clear explanation of the risk factors.
3. Core AI Algorithms Driving Revenue Cycle Automation
To build or deploy an enterprise-grade claim prevention platform, engineering and RCM teams leverage specific, highly optimized machine learning models. Understanding these underlying algorithmic architectures explains how the technology delivers consistent results.
1. Supervised Learning for Binary Classification
At the core of predictive denial scoring is binary classification: determining whether a claim will be approved (0) or denied (1). Healthcare developers frequently utilize Gradient Boosted Decision Trees (GBDT), specifically implementations like XGBoost or LightGBM, due to their exceptional ability to handle tabular, heterogeneous healthcare data.
The model minimizes a log-loss objective function, optimizing parameters across historical features. The final predictive probability $P(\text{Denial} \mid X)$ for a given claim vector $X$ is mathematically formulated as:
$$P(\text{Denial} \mid X) = \frac{1}{1 + e^{-\sum_{k=1}^{K} f_k(X)}}$$
Where each $f_k$ represents an individual decision tree that learns to correct the errors of the preceding trees. This method allows the algorithm to detect complex, non-linear relationships—such as how a specific modifier behaves uniquely when paired with an exact payer-CPT combination.
2. Deep Learning and Transformers for Clinical NLP
To parse complex clinical narratives, advanced systems utilize domain-specific transformer architectures, such as Clinical-BERT or BioBERT. These models are pre-trained on massive corpora of medical literature and clinical records, allowing them to comprehend context, synonyms, and clinical intent.
When an AI evaluates a patient record for medical necessity, the transformer model processes the text through multi-head self-attention mechanisms. This allows it to link distant tokens—such as connecting a documented symptom mentioned on page one of a clinical note with a medical procedure ordered on page four—ensuring the claim meets the exact diagnostic criteria required by the payer.
3. Reinforcement Learning for Autonomous Agent Routing
Once a risk is identified or a denial is received, multi-agent AI systems must determine the optimal resolution pathway. Platforms leverage Reinforcement Learning from Human Feedback (RLHF) to train autonomous software agents.
The agent receives a positive reward when its chosen action—such as selecting a specific appeal template or routing a claim back to a particular coding queue—results in a fast, successful payment.
Over millions of iterations, the agent learns the most efficient path to resolution, minimizing human touchpoints and significantly lowering administrative costs.
4. Real-World Case Studies: From Rejections to Approvals
The practical impact of this technology is best understood through real-world applications. Below are detailed, verified operational examples of how leading healthcare delivery networks implemented AI to reverse rising denial rates.
Case Study 1: Large Health System Confronts Eligibility and Prior Authorization Rejections
A multi-hospital health system with over 450 integrated provider locations was struggling with a rising initial claim denial rate, which had climbed to 13.2%. An internal audit revealed that 42% of these rejections stemmed from front-end issues: inactive insurance coverage on the date of service and missing or unlinked prior authorization numbers.
The AI Intervention
The health system deployed browser-native autonomous AI agents integrated directly into their scheduling software and EHR.
- Real-Time Verification: At the moment a patient schedules an appointment, and again at midnight prior to the clinical encounter, the AI agents automatically query payer portals using secure credential vaulting. They instantly verify active coverage, coordination of benefits (COB), and specific plan exclusions.
- Algorithmic Matching: For specialized imaging and elective surgeries, an AI rules engine cross-references the ordered CPT codes against a dynamically updated database of payer authorization requirements.
- Autonomous Retrieval: If an authorization is required, the AI agent searches the payer portal, retrieves the approved authorization number, and automatically writes it into the appropriate field (Loop 2300 of the 837 claim file) without human intervention.
The Financial and Operational Results
Within 90 days of deploying the autonomous AI workflow, the results demonstrated a clear operational turnaround:
| Performance Metric | Pre-AI Implementation | 90 Days Post-AI | Net Impact |
| Initial Claim Denial Rate | 13.2% | 4.8% | 63.6% Reduction |
| Eligibility-Related Denials | 5.5% | 0.8% | 85.4% Drop |
| Monthly A/R Write-Offs | $1.4M | $310K | $1.09M Saved / Mo. |
| First-Pass Yield (FPY) Rate | 86.8% | 95.2% | 9.6% Increase |
Case Study 2: Academic Medical Center Eliminates Clinical Documentation and Coding Gaps
A major academic medical center experienced declining patient revenue due to rising clinical denials from commercial insurers and Medicare Advantage plans. Key denial drivers included level-of-care mismatches and incorrect coding modifiers for complex orthopedic and cardiovascular procedures.
The AI Intervention
The organization integrated an NLP-driven predictive denial prevention layer directly into its mid-revenue cycle workflow.
- Point-of-Charge Scraping: Immediately after an operative report is completed, AI-powered NLP scans the text and extracts key anatomy, procedure, and implant details.
- Modifier Optimization: A machine learning model compares the extracted clinical details with historical billing patterns. If a surgeon performs bilateral procedures but the coding queue fails to append Modifier -50, the AI flags the omission and routes the claim back to coding with a detailed rationale.
- Payer Policy Alignment: The system continuously updates its internal library by parsing thousands of incoming provider remittance advices. This allows the AI to learn exactly which documentation phrasing leads to successful medical necessity approvals for specific payers.
The Financial and Operational Results
The deployment of the predictive coding and documentation AI delivered significant improvements within six months:
- Coding Denial Reduction: Rejections driven by incorrect modifiers or diagnosis-to-procedure mismatches decreased by 58%.
- Rework Cost Savings: The average cost to process a claim dropped from a manual baseline of $42.50 down to $11.10, driven by the elimination of manual auditing and duplicate efforts.
- Cash Flow Acceleration: The institution’s overall Days Sales Outstanding (DSO) dropped by 6.4 days, injecting millions in liquid capital back into operations.
- Staff Utilization Efficiency: Revenue cycle staff transitioned from manually reviewing every claim to managing only the top 5% highest-risk exceptions highlighted by the AI dashboard.
5. Enterprise Implementation Playbook: A Structured Strategy
For healthcare financial leaders and operations executives, transitioning to an AI-powered denial prevention model requires a methodical, low-risk approach. Below is a structured playbook designed to deliver measurable results quickly.
┌─────────────────────────────────────────────────────────┐
│ WEEK 1: Baseline Assessment & Data Ingestion │
│ ↳ Extract 24 months of 837 (claims) & 835 (remittances) │
└────────────────────────────┬────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ WEEK 2: Model Configuration & Pilot Lane Selection │
│ ↳ Target high-volume, rule-driven segment (e.g., Elg.) │
└────────────────────────────┬────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ WEEK 3: Shadow Mode & Threshold Tuning │
│ ↳ Score live claims in background; calibrate false pos. │
└────────────────────────────┬────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ WEEK 4: Production Go-Live & Human-in-the-Loop │
│ ↳ Route high-risk claims to specialized review queues │
└─────────────────────────────────────────────────────────┘
Baseline Assessment and Data Ingestion (Week 1) – Phase 1
- Extract Historical Records: Securely extract 24 months of historical 837 claim submission files and corresponding 835 Electronic Remittance Advices.
- Establish Key Performance Indicators: Calculate your precise baseline metrics: current initial denial rate, cost per rework, average days in A/R, and your true write-off leakage percentage.
- Map System Infrastructure: Identify all critical endpoints requiring AI connectivity, including your core EHR systems, practice management platforms, and clearinghouse routing nodes.
Model Configuration and Pilot Lane Selection (Week 2) – Phase 2
Isolate High-Volume Segments: Do not attempt to automate the entire revenue cycle at once. To begin with, select a high-volume, rule-based denial category, such as eligibility-related rejections from your largest commercial payer. This approach not only simplifies implementation but also enables faster validation, clearer performance measurement, and more immediate ROI.
- Define Exception Taxonomy: Clearly identify which cases require human review and which can be handled autonomously by AI. Configure Credential Vaults: Establish secure, HIPAA-compliant credential storage for automated access to payer portals.
Shadow Mode and Threshold Tuning (Week 3) – Phase 3
- Execute Background Ingestion: Run the AI predictive scoring engine in “shadow mode” behind your active production environment. Allow the algorithm to evaluate live claims without disrupting your standard billing workflow.
- Calibrate Score Thresholds: Review initial outputs to tune performance.
- Optimize Thresholds: Adjust risk thresholds to reduce false positives and prevent overwhelming staff with low-risk claim reviews. Validate Integrations: Ensure data is written back to the EHR accurately, securely, and without causing field conflicts.
Production Go-Live and Scale (Week 4+) – Phase 4
- Activate Live Routing: Route live claims through the AI prevention engine. Direct all clean, low-risk submissions straight to the clearinghouse while automatically steering high-risk claims into specialized staff queues.
- Implement Continuous Feedback Loops: Establish a daily loop where human coders review and resolve exceptions. The AI model analyzes these manual corrections, updating its predictive algorithms to improve long-term accuracy.
- Expand Operational Scope: Once your pilot lane achieves its target yield, systematically introduce additional payers, complex diagnostic specialties, and advanced clinical documentation review workflows into the AI ecosystem.
6. Addressing Key Challenges: Security, Integration, and Change Management
While the financial benefits of AI adoption are substantial, healthcare organizations frequently encounter operational hurdles during deployment. Navigating these challenges effectively requires a proactive strategy.
Data Security and HIPAA Compliance
Processing Protected Health Information (PHI) within machine learning models demands strict adherence to regulatory standards.
- Business Associate Agreements (BAAs): Ensure all AI vendors and LLM providers sign BAAs to comply with patient privacy regulations. Data Minimization: Share only the data necessary for risk assessment and avoid exposing unnecessary patient identifiers. Encryption: Protect all data with strong encryption standards, including TLS 1.3 in transit and AES-256 at rest.
Overcoming Legacy System Resistance
Many hospital IT departments are hesitant to modify legacy RCM setups due to concerns about workflow disruptions.
To address this resistance, focus on deploying non-invasive AI technologies. Modern browser-native AI agents operate directly within existing user interfaces. They log into portals and enter data exactly like a human specialist, completely eliminating the need for complex, costly HL7 or FHIR API developments that can strain IT resources.
Managing Staff Transformed Workflows
A common point of friction during deployment is staff concern regarding automation and job displacement.
Frame the AI implementation as an optimization tool rather than a replacement strategy. Explain that the automation handles repetitive, administrative data entry tasks, freeing up billing specialists to focus on higher-value responsibilities. These include resolving complex clinical appeals and conducting direct, high-touch peer-to-peer discussions with payers.
7. The Future of AI in Healthcare Revenue Protection
The evolution of automated revenue cycle management is moving rapidly beyond simple denial resolution toward comprehensive, end-to-end revenue protection.
[2024: Reactive Resolution] ──> [2026: Predictive Prevention] ──> [2028+: Autogenous Contracting]
Manual Appeal Rework Pre-Submission Risk Scoring Real-Time Adjudication & Smart Contracts
We are entering an era of truly autonomous RCM networks. In this landscape, multi-agent AI systems representing provider networks will communicate directly with parallel AI models deployed by insurance payers. Claims will be evaluated, adjusted, and fully adjudicated in real time at the exact moment care is delivered, making the traditional 90-day accounts receivable cycle obsolete.
Furthermore, as generative AI models advance, platforms will go beyond simply flagging omissions. They will autonomously draft comprehensive, legally precise appeal packages. These systems automatically combine clinical notes, historical precedents, and contract terms into comprehensive documents, delivering results faster and at a scale beyond manual teams.
For healthcare enterprises aiming to protect their net margins, adopting predictive AI is no longer optional. Embracing algorithmic claim prevention allows organizations to eliminate administrative waste, accelerate cash conversion, and ensure that medical teams are fully reimbursed for the essential care they deliver.
Frequently Asked Questions
What is the average claim denial rate for healthcare providers?
The national average initial claim denial rate stands at approximately 11.8%, according to comprehensive industry benchmarks. While leading healthcare organizations maintain first-pass denial rates below 5%, many legacy health systems experience denial rates exceeding 10% due to inefficient manual billing processes.
How does predictive analytics prevent medical claim denials?
Predictive analytics uses machine learning trained on millions of claims to assess denial risk before submission, enabling teams to identify and correct errors proactively.
Can AI systems integrate with existing EHR platforms like Epic or Cerner?
Yes. Modern AI denial prevention solutions offer flexible deployment models. These platforms integrate with EHR systems through secure HL7/FHIR APIs or use autonomous agents that operate existing interfaces like human users, eliminating the need for custom development.
What are the most common reasons for health insurance claim denials?
The majority of preventable rejections stem from front-end and administrative errors. Common causes include eligibility errors, missing prior authorizations, insufficient clinical documentation, and incorrect coding modifiers.
For a detailed overview of how healthcare organizations are modernizing billing operations with AI-driven workflows, watch this technical session:
Transforming Healthcare Revenue Cycle Management with AI Agents
This video provides an in-depth look at building multi-agent AI architectures designed to automate complex claims processing and denial mitigation while maintaining rigorous compliance standards.